Opinion
Numbers behind different COVID-19 vaccines

By M. C. M. Iqbal
The vaccines against COVID-19, available today, are based on different strategies and come with different numbers to indicate their performance. Many of us wish to know if one vaccine is better than the other. Two concepts underlying the performance of the vaccines are efficacy and effectiveness. The Pfizer-BioNTech vaccine has an efficacy of 95 percent, the Moderna Vaccine is 94.5 percent and the Russian made Sputnik vaccine is over 90 percent. Does this mean some vaccines are better than the other? The short answer is no. All the approved vaccines are equally good. So, let us look at what these numbers mean.
These numbers refer to statistical calculations to interpret the results of vaccination trials conducted by the manufacturers of vaccines, following a prescribed format. The method of calculation was developed over 100 years ago by two statisticians, who published their results in the Proceedings of the Royal Society of Medicine in 1915. They, Major Greenwood (Major is his first name and not a military title) and Udny Yule, were tasked with interpreting the results of immunization of British soldiers against typhoid and cholera, who were fighting in different regions of Europe and Asia favourable to the development of cholera epidemics. In a paper stretching over 82 pages, the authors developed the theoretical and mathematical background for calculating the efficacy of vaccines.
This article seeks to explain to the lay reader what these numbers imply and to bring out the differences between efficacy and effectiveness of a vaccine.
Efficacy and effectiveness
At first sight these two terms appear to be synonyms. However, in the world of vaccines and medicine, these two terms are not the same. Efficacy of a vaccine is how it performs under ideal and controlled conditions in a clinical trial (see below). During clinical trials, the outcome of vaccination is compared between a group of vaccinated people and another group given an inactive form of the vaccine (called a placebo). The effectiveness of a vaccine is how the vaccine performs in the real world – that is after the vaccine is approved by the regulatory agencies and you and I are vaccinated.
The efficacy of a vaccine is measured by the manufacturers under ideal conditions in a clinical trial where criteria are specified for selecting and excluding volunteers. These criteria are usually age groups, gender, ethnicity, geographical location and socio-economic standing. If the criteria are specific, then the effects of the vaccine or drug would not be applicable across the population. For example, if the COVID-19 vaccines are not tested on children below 18 years, then the approved vaccine cannot be used on children.
The effectiveness of a drug or vaccine is a measure of how well the drug or vaccine performs in real life, in a diverse population: Fitness geeks and couch potatoes, housewives and nurses, and farmers and office workers. Effectiveness is of relevance to the medical community and healthcare authorities who are treating the patients. Thus, studies on effectiveness would look at to what extent the vaccine is beneficial to the patient to prevent infection.
One may ask, why not simply look at the effectiveness of the vaccine? This is because if the participants in an initial trial of the vaccine are not carefully controlled, then it is difficult to interpret the outcome of the trial. We have many characteristics, which can potentially interfere with the outcome of a trial testing a vaccine. The person volunteering for the trial could be young or old, pregnant or not, a marathon runner or an average person and smoker or non-smoker. Thus, the volunteers selected for the trials are very similar within their groups with many criteria to exclude persons who could confuse the results (for example, an unhealthy person with other diseases would be excluded).
Efficacy of a vaccine asks the question ‘Does the vaccine work under ideal conditions?’ On the other hand, a study on the effectiveness of the same vaccine asks the question ‘Does vaccination work in the real world?’
Clinical trials
Under normal circumstances, vaccines take many years of research and testing to be approved. The COVID-19 pandemic was unprecedented, and pharmaceutical companies embarked on a race against time to produce safe and effective vaccines. The genome of this coronavirus, which was discovered by Chinese scientists, in January 2020, was a major contribution to the development of the vaccines. At the moment there are 94 vaccines being tested on humans in clinical trials, 32 of which have reached the final stage of Phase 3 testing.
To obtain approval for a vaccine, the vaccine manufacturers go through a prescribed process to ensure that the vaccine is safe. All the countries have a national drug approval agency, who should approve the use of a drug or vaccine in that country. The Food and Drug Administration (FDA) in the United States is an important regulatory agency, which has stringent criteria to approve medicines and drugs. In Sri Lanka, it is the National Medicines Regulatory Authority. COVID-19 vaccines are also assessed and approved by the WHO.
Initially, the vaccine is tested on cells in the laboratory and then given to animals, usually mice or monkeys. After this, if the mice or monkeys are happy, human volunteers are recruited to conduct the clinical trials, which is done in three phases. In the first phase, the vaccine is tested on a small group of people to determine the safety, dosage and ability to stimulate our immune system. If this is confirmed, the vaccine then moves into the Phase 2 stage where the safety of the vaccine is tested on hundreds of people who are split into different groups. Once these trials are successful, the vaccine moves to the final Phase 3 trials. Here thousands of people are recruited as volunteers. For the Pfizer-BioNTech vaccine there were over 40,000 volunteers, above the age of 16, from different countries. This trial is more comprehensive, with the volunteers belonging to different age groups, physical fitness, ethnicities and geographical locations. The volunteers are divided into two groups. One group gets the real vaccine while the other group gets a fake vaccine or placebo (the syringe has just water). The volunteers would not know if he/she is getting the vaccine or a placebo and neither do the nurses and doctors giving the vaccine. This is called a double-blind clinical trial. Thus, no one knows, except those conducting the trial, who was vaccinated with what.
After some time, the volunteers, who fell sick with the coronavirus, are PCR tested to confirm if they are COVID-19 positive. The scientists will be on the lookout for any side effects of the vaccine; if they find any cause for concern the trial can be stopped temporarily to conduct investigations and remedy the problem. If the scientists are not satisfied, the trial would be abandoned. Once the results are in, the calculations are done, and all the details are submitted to the regulating authorities. The regulators would ask the manufacturers more questions and once they are satisfied, approval is given to manufacture and market the vaccine. To accelerate the process, such as now during the COVID-19 crises, Phase 1 and 2 may be combined and run in parallel.
Calculating efficacy
The calculations involved are quite simple once the data is collected. Let us assume that 50,000 volunteers were recruited for the vaccination trial. Half were given the vaccine and the other half a placebo. Let us assume that of the 25,000 who received the vaccine, 10 persons were infected, and of the other 25,000 who received the placebo, 200 were infected. Although the numbers of people infected are small, those in the placebo group are 20 times larger (see Table). The researchers are concerned with the relative risk between the groups. This is called the efficacy of the vaccine.
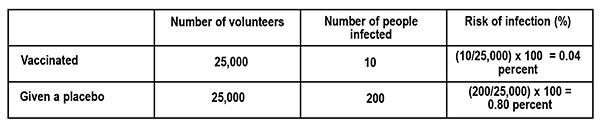
The risk of infection is calculated as follows.
What is the difference in the risk of infection between the vaccinated group and those who got the placebo? From the table this is, 0.80 percent – 0.04 percent = 0.76 percent.
Thus, the vaccine reduced the risk of infection by 0.76 percent, which looks quite small. This is what would happen if we are vaccinated. To understand this in terms of the risk of infection, if none were vaccinated, we look at the ratio of the Reduction in Infection (0.76 percent) to the Risk of infection (0.80 percent – those who got the fake vaccine). This is the Vaccine Efficacy (VE).
VE percent = Reduction in infection ÷ Risk of infection = 0.76 ÷ 0.80 = 95 percent
If this is still confusing, let us see what it means in a population of 100,000 persons who are vaccinated with a vaccine of 95 percent efficacy, and exposed to the virus. From the table above, the risk of infection for the vaccinated population is 0.04 percent, which translates to 40 persons (0.04 percent x 100,000). That is, we can expect that 40 persons would fall ill with an infection by the coronavirus and the rest of the vaccinated people may not develop an infection at all or develop an asymptomatic infection (you are infected but do not show symptoms) or get a mild disease.
(This example of calculating Vaccine Efficacy is adapted from an article by Dashiell Young-Saver in the New York Times of December 13, 2020, where the above calculation is explained in detail for students.)
What does efficacy mean?
The efficacy of a vaccine refers to two aspects. The first is how many of us are protected by the vaccine if we are exposed to the virus; this is given by the percentage. The vaccine also refers to different disease conditions it is capable of preventing. This could be causing an infection, mild disease, severe disease, hospitalisation, or death. This information can be found if one looks carefully at the statements issued by the vaccine manufacturer and regulatory agencies. For example, the statement by Pfizer-BioNTech states: Pfizer-BioNTech COVID-19 vaccine, BNT162b2, was 91.3 percent effective against COVID-19 (symptomatic cases of COVID-19), measured seven days through up to six months after the second dose. The vaccine was 100 percent effective against severe disease as defined by the US centres for Disease Control and Prevention (CDC), and 95.3 percent effective against severe disease as defined by the US FDA.
The efficacy of a vaccine (VE) is the relative reduction of being infected, if we are vaccinated, compared to the placebo or unvaccinated group. If the vaccine is perfect, then the risk of being infected is totally eliminated, so that VE = 1 or it is 100 percent. On the other hand, if there is no difference in the number of people infected between the two groups, the vaccine has no efficacy, or it is zero. Even with a perfect vaccine, our capacity to acquire an infection is determined by our age, health and immunity status.
In short, efficacy is a statistical measurement based on clinical trials of the vaccine’s ability to prevent infection. The volunteers taking part in the trials are not a perfect sample or representative of the real world (for example, children and sick people do not take part). Is there a lower limit for the efficacy of a vaccine to be accepted? Under the present circumstances, the FDA said it would consider granting emergency approval if the vaccines showed even 50 percent efficacy; the vaccines that have received approval now show an efficacy of over 90 percent.
Effectiveness
The effectiveness of the vaccine tells us how well the vaccine is performing among the population, in the real world, to prevent infection. The effectiveness of the vaccine depends on the impact it makes on society. After vaccination our immune system is primed to combat the coronavirus, reducing the multiplication of the virus in our body. This will gradually slow down the spread of the virus as more and more people are vaccinated. In other words, it is important that most if not all the people are vaccinated to have a large impact on the spread of the virus in society. Good examples are the smallpox vaccine, which completely eliminated the smallpox virus, and the polio vaccine, which has almost wiped out the polio virus except for a few small pockets in Pakistan, Afghanistan and Africa. Thus, the effectiveness of a vaccine looks at the medical and societal importance of the outcome.
Here is the above in a nutshell. The percentage numbers given with a vaccine refers to its efficacy – its ability to prevent an infection developing into a serious condition, determined under controlled clinical trials. Vaccines do not prevent infection – they prevent the infection from developing into a severe disease. Once we are vaccinated, our immune system is activated. If we are infected by the coronavirus, the virus has a small window of time to multiply, before it is eliminated by our immune system. This means we can release virus particles from our body, but much less than if we were not vaccinated. The message is we should get vaccinated with the first available vaccine and still wear our masks when going outside, even if we are vaccinated. The chances of ending up in a hospital is low and the chances of ending up in the ICU is very low. There is always a chance.
‘Tis impossible to be sure of anything but Death and Taxes (Christopher Bullock, 1716).
(M.C.M. Iqbal is Associate Research professor, Plant and Environmental Science, National Institute of Fundamental Studies, Hanthane Road, Kandy, and can be reached at iqbal.mo@nifs.ac.lk)
References
Zimmer, C. New York Times Nov. 20, 2020. Two companies say their vaccines are 95 percent effective. What does that mean?
Haelle,T. Association of Health Care Journalists. October 22, 2020. Know the nuances of vaccine efficacy when covering Covid-19 trials. https://healthjournalism.org/blog/2020/10/know-the-nuances-of-vaccine-efficacy-when-covering-covid-19-vaccine-trials/
Greenwood, M., & Yule, G. U. (1915). The Statistics of Anti-typhoid and Anti-cholera Inoculations, and the Interpretation of such Statistics in general. Proceedings of the Royal Society of Medicine, 8 (Sect Epidemiol State Med), 113–194.
Food and Drug Administration, US Department of Health and Human Services. https://www.fda.gov/media/139638/download

 by Dr B.J.C.Perera
by Dr B.J.C.Perera
MBBS(Cey), DCH(Cey), DCH(Eng), MD(Paed), MRCP(UK), FRCP(Edin),
FRCP(Lon), FRCPCH(UK), FSLCPaed, FCCP, Hony FRCPCH(UK), Hony. FCGP(SL)
Specialist Consultant Paediatrician and Honorary Senior Fellow,
Postgraduate Institute of Medicine, University of Colombo, Sri Lanka.
Joint Editor, Sri Lanka Journal of Child Health
In an age of unprecedented global development, technological advancements, universal connectivity, and improvements in living standards in many areas of the world, it is a very dark irony that child food poverty remains a pressing issue. UNICEF defines child food poverty as children’s inability to access and consume a nutritious and diverse diet in early childhood. Despite the planet Earth’s undisputed capacity to produce enough food to nourish everyone, millions of children still go hungry each day. We desperately need to explore the multifaceted deleterious effects of child food poverty, on physical health, cognitive development, emotional well-being, and societal impacts and then try to formulate a road map to alleviate its deleterious effects.
Every day, right across the world, millions of parents and families are struggling to provide nutritious and diverse foods that young children desperately need to reach their full potential. Growing inequities, conflict, and climate crises, combined with rising food prices, the overabundance of unhealthy foods, harmful food marketing strategies and poor child-feeding practices, are condemning millions of children to child food poverty.
In a communique dated 06th June 2024, UNICEF reports that globally, 1 in 4 children; approximately 181 million under the age of five, live in severe child food poverty, defined as consuming at most, two of eight food groups in early childhood. These children are up to 50 per cent more likely to suffer from life-threatening malnutrition. Child Food Poverty: Nutrition Deprivation in Early Childhood – the third issue of UNICEF’s flagship Child Nutrition Report – highlights that millions of young children are unable to access and consume the nutritious and diverse diets that are essential for their growth and development in early childhood and beyond.
It is highlighted in the report that four out of five children experiencing severe child food poverty are fed only breastmilk or just some other milk and/or a starchy staple, such as maize, rice or wheat. Less than 10 per cent of these children are fed fruits and vegetables and less than 5 per cent are fed nutrient-dense foods such as eggs, fish, poultry, or meat. These are horrendous statistics that should pull at the heartstrings of the discerning populace of this world.
The report also identifies the drivers of child food poverty. Strikingly, though 46 per cent of all cases of severe child food poverty are among poor households where income poverty is likely to be a major driver, 54 per cent live in relatively wealthier households, among whom poor food environments and feeding practices are the main drivers of food poverty in early childhood.
One of the most immediate and visible effects of child food poverty is its detrimental impact on physical health. Malnutrition, which can result from both insufficient calorie intake and lack of essential nutrients, is a prevalent consequence. Chronic undernourishment during formative years leads to stunted growth, weakened immune systems, and increased susceptibility to infections and diseases. Children who do not receive adequate nutrition are more likely to suffer from conditions such as anaemia, rickets, and developmental delays.
Moreover, the lack of proper nutrition can have long-term health consequences. Malnourished children are at a higher risk of developing chronic illnesses such as heart disease, diabetes, and obesity later in life. The paradox of child food poverty is that it can lead to both undernutrition and overnutrition, with children in food-insecure households often consuming calorie-dense but nutrient-poor foods due to economic constraints. This dietary pattern increases the risk of obesity, creating a vicious cycle of poor health outcomes.
The impacts of child food poverty extend beyond physical health, severely affecting cognitive development and educational attainment. Adequate nutrition is crucial for brain development, particularly in the early years of life. Malnutrition can impair cognitive functions such as attention, memory, and problem-solving skills. Studies have consistently shown that malnourished children perform worse academically compared to their well-nourished peers. Inadequate nutrition during early childhood can lead to reduced school readiness and lower IQ scores. These children often struggle to concentrate in school, miss more days due to illness, and have lower overall academic performance. This educational disadvantage perpetuates the cycle of poverty, as lower educational attainment reduces future employment opportunities and earning potential.
The emotional and psychological effects of child food poverty are profound and are often overlooked. Food insecurity creates a constant state of stress and anxiety for both children and their families. The uncertainty of not knowing when or where the next meal will come from can lead to feelings of helplessness and despair. Children in food-insecure households are more likely to experience behavioural problems, including hyperactivity, aggression, and withdrawal. The stigma associated with poverty and hunger can further exacerbate these emotional challenges. Children who experience food poverty may feel shame and embarrassment, leading to social isolation and reduced self-esteem. This psychological toll can have lasting effects, contributing to mental health issues such as depression and anxiety in adolescence and adulthood.
Child food poverty also perpetuates cycles of poverty and inequality. Children who grow up in food-insecure households are more likely to remain in poverty as adults, continuing the intergenerational transmission of disadvantage. This cycle of poverty exacerbates social disparities, contributing to increased crime rates, reduced social cohesion, and greater reliance on social welfare programmes. The repercussions of child food poverty ripple through society, creating economic and social challenges that affect everyone. The healthcare costs associated with treating malnutrition-related illnesses and chronic diseases are substantial. Additionally, the educational deficits linked to child food poverty result in a less skilled workforce, which hampers economic growth and productivity.
Addressing child food poverty requires a multi-faceted approach that tackles both immediate needs and underlying causes. Policy interventions are crucial in ensuring that all children have access to adequate nutrition. This can include expanding social safety nets, such as food assistance programmes and school meal initiatives, as well as targeted manoeuvres to reach more vulnerable families. Ensuring that these programmes are adequately funded and effectively implemented is essential for their success.
In addition to direct food assistance, broader economic and social policies are needed to address the root causes of poverty. This includes efforts to increase household incomes through living wage policies, job training programs, and economic development initiatives. Supporting families with affordable childcare, healthcare, and housing can also alleviate some of the financial pressures that contribute to food insecurity.
Community-based initiatives play a vital role in combating child food poverty. Local food banks, community gardens, and nutrition education programmes can help provide immediate relief and promote long-term food security. Collaborative efforts between government, non-profits, and the private sector are necessary to create sustainable solutions.
Child food poverty is a profound and inescapable issue with far-reaching consequences. Its deleterious effects on physical health, cognitive development, emotional well-being, and societal stability underscore the urgent need for comprehensive action. As we strive for a more equitable and just world, addressing child food poverty must be a priority. By ensuring that all children have access to adequate nutrition, we can lay the foundation for a healthier, more prosperous future for individuals and society as a whole. The fight against child food poverty is not just a moral imperative but an investment in our collective future. Healthy, well-nourished children are more likely to grow into productive, contributing members of society. The benefits of addressing this issue extend beyond individual well-being, enhancing economic stability and social harmony. It is incumbent upon us all to recognize and act upon the understanding that every child deserves the right to adequate nutrition and the opportunity to thrive.
Despite all of these existent challenges, it is very definitely possible to end child food poverty. The world needs targeted interventions to transform food, health, and social protection systems, and also take steps to strengthen data systems to track progress in reducing child food poverty. All these manoeuvres must comprise a concerted effort towards making nutritious and diverse diets accessible and affordable to all. We need to call for child food poverty reduction to be recognized as a metric of success towards achieving global and national nutrition and development goals.
Material from UNICEF reports and AI assistance are acknowledged.
By Dr Upul Wijayawardhana
The colossal failure of not a single opinion poll predicting accurately the result of the Indian parliamentary election, the greatest exercise in democracy in the world, raises the question whether the importance of opinion polls is vastly exaggerated. During elections two types of opinion polls are conducted; one based on intentions to vote, published during or before the campaign, often being not very accurate as these are subject to many variables but exit polls, done after the voting where a sample tally of how the voters actually voted, are mostly accurate. However, of the 15 exit polls published soon after all the votes were cast in the massive Indian election, 13 vastly overpredicted the number of seats Modi’s BJP led coalition NDA would obtain, some giving a figure as high as 400, the number Modi claimed he is aiming for. The other two polls grossly underestimated predicting a hung parliament. The actual result is that NDA passed the threshold of 272 comfortably, there being no landslide. BJP by itself was not able to cross the threshold, a significant setback for an overconfident Mody! Whether this would result in less excesses on the part of Modi, like Muslim-bashing, remains to be seen. Anyway, the statement issued by BJP that they would be investigating the reasons for failure rather than blaming the process speaks very highly of the maturity of the democratic process in India.
I was intrigued by this failure of opinion polls as this differs dramatically from opinion polls in the UK. I never failed to watch ‘Election night specials’ on BBC; as the Big Ben strikes ‘ten’ (In the UK polls close at 10pm} the anchor comes out with “Exit polls predict that …” and the actual outcome is often almost as predicted. However, many a time opinion polls conducted during the campaign have got the predictions wrong. There are many explanations for this.
An opinion poll is defined as a research survey of public opinion from a particular sample, the origin of which can be traced back to the 1824 US presidential election, when two local newspapers in North Carolina and Delaware predicted the victory of Andrew Jackson but the sample was local. First national survey was done in 1916 by the magazine, Literary Digest, partly for circulation-raising, by mailing millions of postcards and counting the returns. Of course, this was not very scientific though it accurately predicted the election of Woodrow Wilson.
Since then, opinion polls have grown in extent and complexity with scientific methodology improving the outcome of predictions not only in elections but also in market research. As a result, some of these organisations have become big businesses. For instance, YouGov, an internet-based organisation co-founded by the Iraqi-born British politician Nadim Zahawi, based in London had a revenue of 258 million GBP in 2023.
In Sri Lanka, opinion polls seem to be conducted by only one organisation which, by itself, is a disadvantage, as pooled data from surveys conducted by many are more likely to reflect the true situation. Irrespective of the degree of accuracy, politicians seem to be dependent on the available data which lend explanations to the behaviour of some.
The Institute for Health Policy’s (IHP) Sri Lanka Opinion Tracker Survey has been tracking the voting intentions for the likely candidates for the Presidential election. At one stage the NPP/JVP leader AKD was getting a figure over 50%. This together with some degree of international acceptance made the JVP behave as if they are already in power, leading to some incidents where their true colour was showing.
The comments made by a prominent member of the JVP who claimed that the JVP killed only the riff-raff, raised many questions, in addition to being a total insult to many innocents killed by them including my uncle. Do they have the authority to do so? Do extra-judicial killings continue to be JVP policy? Do they consider anyone who disagrees with them riff-raff? Will they kill them simply because they do not comply like one of my admired teachers, Dr Gladys Jayawardena who was considered riff-raff because she, as the Chairman of the State Pharmaceutical Corporation, arranged to buy drugs cheaper from India? Is it not the height of hypocrisy that AKD is now boasting of his ties to India?
Another big-wig comes with the grand idea of devolving law and order to village level. As stated very strongly, in the editorial “Pledges and reality” (The Island, 20 May) is this what they intend to do: Have JVP kangaroo-courts!
Perhaps, as a result of these incidents AKD’s ratings has dropped to 39%, according to the IHP survey done in April, and Sajith Premadasa’s ratings have increased gradually to match that. Whilst they are level pegging Ranil is far behind at 13%. Is this the reason why Ranil is getting his acolytes to propagate the idea that the best for the country is to extend his tenure by a referendum? He forced the postponement of Local Governments elections by refusing to release funds but he cannot do so for the presidential election for constitutional reasons. He is now looking for loopholes. Has he considered the distinct possibility that the referendum to extend the life of the presidency and the parliament if lost, would double the expenditure?
Unfortunately, this has been an exercise in futility and it would not be surprising if the next survey shows Ranil’s chances dropping even further! Perhaps, the best option available to Ranil is to retire gracefully, taking credit for steadying the economy and saving the country from an anarchic invasion of the parliament, rather than to leave politics in disgrace by coming third in the presidential election. Unless, of course, he is convinced that opinion polls do not matter and what matters is the ballots in the box!

By Prof. Kirthi Tennakone
ktenna@yahoo.co.uk
Thoughtfulness is the quality of being conscious of issues that arise and considering action while seeking explanations. It facilitates finding solutions to problems and judging experiences.
Almost all human accomplishments are consequences of thoughtfulness.
Can you perform day-to-day work efficiently and effectively without being thoughtful? Obviously, no. Are there any major advancements attained without thought and contemplation? Not a single example!
Science and technology, art, music and literary compositions and religion stand conspicuously as products of thought.
Thought could have sinister motives and the only way to eliminate them is through thought itself. Thought could distinguish right from wrong.
Empathy, love, amusement, and expression of sorrow are reflections of thought.
Thought relieves worries by understanding or taking decisive action.
Despite the universal virtue of thoughtfulness, some advocate an idea termed mindfulness, claiming the benefits of nurturing this quality to shape mental wellbeing. The concept is defined as focusing attention to the present moment without judgment. A way of forgetting the worries and calming the mind – a form of meditation. A definition coined in the West to decouple the concept from religion. The attitude could have a temporary advantage as a method of softening negative feelings such as sorrow and anger. However, no man or woman can afford to be non-judgmental all the time. It is incompatible with indispensable thoughtfulness! What is the advantage of diverting attention to one thing without discernment during a few tens of minute’s meditation? The instructors of mindfulness meditation tell you to focus attention on trivial things. Whereas in thoughtfulness, you concentrate the mind on challenging issues. Sometimes arriving at groundbreaking scientific discoveries, solution of mathematical problems or the creation of masterpieces in engineering, art, or literature.
The concept of meditation and mindfulness originated in ancient India around 1000 BCE. Vedic ascetics believed the practice would lead to supernatural powers enabling disclosure of the truth. Failing to meet the said aspiration, notwithstanding so many stories in scripture, is discernable. Otherwise, the world would have been awakened to advancement by ancient Indians before the Greeks. The latter culture emphasized thoughtfulness!
In India, Buddha was the first to deviate from the Vedic philosophy. His teachers, Alara Kalama and Uddaka Ramaputra, were adherents of meditation. Unconvinced of their approach, Buddha concluded a thoughtful analysis of the actualities of life should be the path to realisation. However, in an environment dominated by Vedic tradition, meditation residually persisted when Buddha’s teachings transformed into a religion.
In the early 1970s, a few in the West picked up meditation and mindfulness. We Easterners, who criticize Western ideas all the time, got exalted after seeing something Eastern accepted in the Western circles. Thereafter, Easterners took up the subject more seriously, in the spirit of its definition in the West.
Today, mindfulness has become a marketable commodity – a thriving business spreading worldwide, fueled largely by advertising. There are practice centres, lessons onsite and online, and apps for purchase. Articles written by gurus of the field appear on the web.
What attracts people to mindfulness programmes? Many assume them being stressed and depressed needs to improve their mental capacity. In most instances, these are minor complaints and for understandable reasons, they do not seek mainstream medical interventions but go for exaggeratedly advertised alternatives. Mainstream medical treatments are based on rigorous science and spell out both the pros and cons of the procedure, avoiding overstatement. Whereas the alternative sector makes unsubstantiated claims about the efficacy and effectiveness of the treatment.
Advocates of mindfulness claim the benefits of their prescriptions have been proven scientifically. There are reports (mostly in open-access journals which charge a fee for publication) indicating that authors have found positive aspects of mindfulness or identified reasons correlating the efficacy of such activities. However, they rarely meet standards normally required for unequivocal acceptance. The gold standard of scientific scrutiny is the statistically significant reproducibility of claims.
If a mindfulness guru claims his prescription of meditation cures hypertension, he must record the blood pressure of participants before and after completion of the activity and show the blood pressure of a large percentage has stably dropped and repeat the experiment with different clients. He must also conduct sessions where he adopts another prescription (a placebo) under the same conditions and compares the results. This is not enough, he must request someone else to conduct sessions following his prescription, to rule out the influence of the personality of the instructor.
The laity unaware of the above rigid requirements, accede to purported claims of mindfulness proponents.
A few years ago, an article published and widely cited stated that the practice of mindfulness increases the gray matter density of the brain. A more recent study found there is no such correlation. Popular expositions on the subject do not refer to the latter report. Most mindfulness research published seems to have been conducted intending to prove the benefits of the practice. The hard science demands doing the opposite as well-experiments carried out intending to disprove the claims. You need to be skeptical until things are firmly established.
Despite many efforts diverted to disprove Einstein’s General Theory of Relativity, no contradictions have been found in vain to date, strengthening the validity of the theory. Regarding mindfulness, as it stands, benefits can neither be proved nor disproved, to the gold standard of scientific scrutiny.
Some schools in foreign lands have accommodated mindfulness training programs hoping to develop the mental facility of students and Sri Lanka plans to follow. However, studies also reveal these exercises are ineffective or do more harm than good. Have we investigated this issue before imitation?
Should we force our children to focus attention on one single goal without judgment, even for a moment?
Why not allow young minds to roam wild in their deepest imagination and build castles in the air and encourage them to turn these fantasies into realities by nurturing their thoughtfulness?
Be more thoughtful than mindful?



US sports envoys to Lanka to champion youth development

Rahuman questions sudden cancellation of leave of CEB employees






